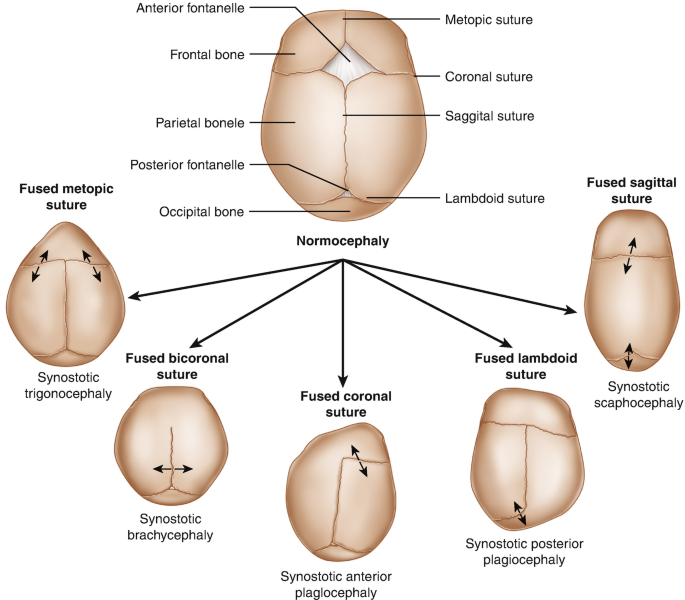
Craniosynostosis
Craniosynostosis occurs due to the premature in-utero fusion of one or more cranial sutures. These sutures allow for passage through the birth canal and, later in development, allow the expansion and growth of the underlying brain. When these sutures close prematurely, the head shape becomes altered depending on the sutures involved. Most cases involve a single suture and are classified as non-syndromic. However, Crouzon, Pfeiffer, and Apert syndromes have been associated with multi-sutural craniosynostosis. The treatment of craniosynostosis involves surgical intervention to unlock the fused sutures, ensuring unrestricted brain development and correcting cosmetic deformities.
Treatment and Managements
The management of craniosynostosis primarily focuses on surgical intervention. For cases involving a single suture, surgery is often performed in an elective manner. However, in cases of multi-sutural involvement, surgery may be expedited if there is concern for elevated intracranial pressure. In cases of sagittal synostosis, spring-mediated cranioplasty may be used in addition to suturectomy.[42][43] A limitation of using springs is the necessity for a second surgery to remove them once the desired head shape is accomplished. Once the child reaches the age of 6 months, endoscopic suturectomy is typically not performed because the skull becomes too hard for postoperative helmeting to be effective. In these cases, more extensive surgeries are required, including cranial vault reconstructions, frontal-orbital advancements, or distraction osteogenesis, depending on the subtype of craniosynostosis.
If patients develop hydrocephalus, treatment options involve either placement of a shunt or endoscopic third ventriculostomy, with or without choroid plexus coagulation.[22] When considering a ventriculoperitoneal shunt, it is essential to consider the need for further open vault reconstructions. Placement of a frontal shunt may result in exposure of the shunt hardware, making a posterior approach potentially more appropriate. If there is a concern for the need for future operations, an endoscopic third ventriculostomy may be a reasonable initial approach.